Introduction to Learning.
Learning is a life long process that has several phases. Most notably a childhood phase. where the teacher's agenda dominates and the adult phase, where the learner is more actively involved. In professional education, the new recruit has often to submit to another phase of teacher dominated education, and this can affect their learning pattern for the rest of the professional life. One of the roles of the postgraduate teacher is to help the learner to assume a more active and responsible role in his or her learning.
The learning of the qualified professional has to satisfy the following broad aims:
- to maintain and consolidate knowledge and skills
- to acquire new appropriate knowledge and skills
- to develop areas of new interest
- to facilitate the process of contributing to new knowledge and skills
The fields within which these general aims will apply will be:
- clinical medicine
- business management
- public health
- education
- health service administration and planning
- science and research
He or she is an adult learner with the characteristics of which are laid out below:
(Knowles M (1984) The Adult Learner – A neglected species)
- respond best to a non-threatening learning environment where there is a good teacher/learner relationship.
- want to assess themselves against a relevant standard to determine educational needs.
- want to select their own learning experiences - self directing.
- prefer a problem orientated patient based approach to learning.
- want to apply their knowledge and skills immediately.
- want to know how they are progressing.
- want to contribute from their own knowledge and skills to help others to learn.
In order to help the individual learner, the mentor will be involved in some of the processes:
1.Negotiating skills
2.Learning styles
3.Needs analysis
4.Planning learning
5.Educational resourcing
6.Evaluating learning
Learning styles
Learning is a characteristic of our species. We all learn, some better than others, some faster than others. The way in which we learn can vary. Kolb defined four main styles of learning: (Experiential Learning Prentice Hall 1984)
1.Concrete experience - feeling - having the experience
2.Reflective observation - watching - reviewing the experience
3.Abstract conceptualisation - thinking - concluding from the experience
4.Active experimentation - doing - planning the next stage
These four styles also form the points on the circumference of the learning cycle.
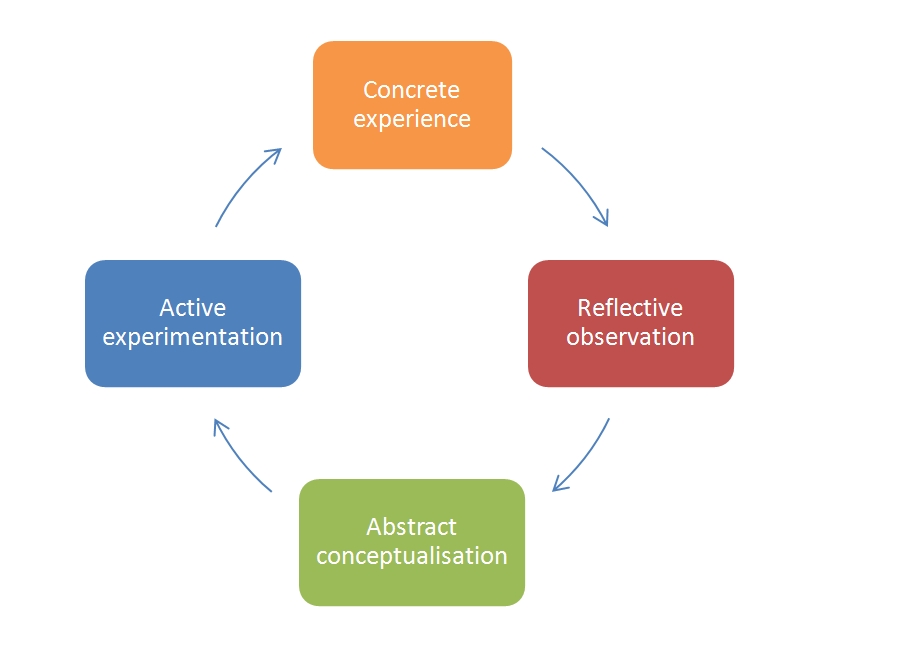
The Kolb model of learning sets the styles round the perimeter of a circle. The process of learning is complete if the learner passes through all the styles.
The complete learner possesses the ability to pass through all the stages with equal facility, but most people have a preferred learning style. The style is preferred or dominant not exclusive. We each enter the circle at the point of our own preference and move according to our needs and circumstances. In some instances, the learner just learns in the one style and sees no need to move. In medicine, this would be difficult, but not impossible.
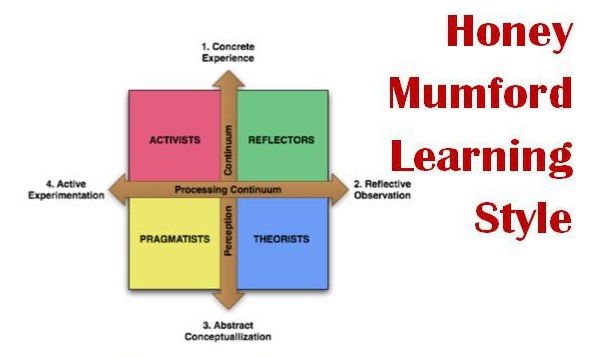
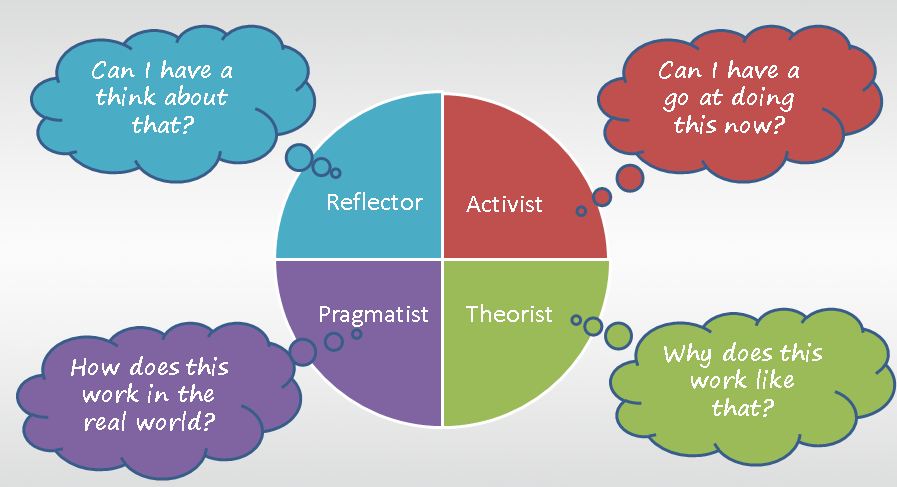
The work and publications of Peter Honey and Alan Mumford have produced a method of exploring the individual's learning style. (The Manual of Learning Styles, P Honey an A Mumford, P Honey Publications, Maidenhead 1992). The questionnaire published in the manual enables the learner to determine their learning style, compare their results with the accumulated results of many thousands, and explore their preferred ways of learning. When describing the styles they use the terms activist, reflector, theorist and pragmatist, corresponding with Kolb's concrete experience, reflective observation, abstract conceptualisation and active experimentation.
Completing the learning style questionnaire enables the learner to select the method most suited to their preferred style. It will also enable them to make the most of that style, and from the basis of success, develop their other styles.
For effective learning to occur, a learner needs to feel comfortable with the method, a personalised plan with the method tailored to the preferred style is likely to achieve this.
The elegance of this model is in its easy adaptation to the problem solving process often used by health care professionals.
Defining learning needs can be difficult, often because we have been educated in the system of always being right and justifying ourselves. The underlying philosophy of defining learning needs is that of the error model, where errors or omissions are not only permitted. but their recognition encouraged and celebrated. In this model, the teacher is the factor that enables the learner to recognise and act on the errors. In medicine, error equates to tragedy and even death. Whilst this can be the case, it is probably a failure to recognise small errors that results in a major error.
The error does not have to be a wrong action, it may be an omission. It is possible to view a referral from general practice as a failure to cope, or an inability to do something. This might be appropriate in the area of major surgery or cardiac investigation, but in some other instances we refer because of a lack of knowledge or skill. Analysis of referral letters often discloses such areas of need. This can be either a personal, practice or other group activity,